
Imagine waking up in a world where sound simply doesn't exist. For people with profound sensorineural hearing loss, traditional hearing aids often feel like trying to use a magnifying glass to see in total darkness-they amplify sound, but if the "sensors" in the ear are broken, amplification does nothing. This is where Cochlear Implants is a medical device that bypasses damaged parts of the inner ear to provide a direct electrical signal to the auditory nerve. Unlike a hearing aid, which makes sound louder, an implant creates a new way for the brain to perceive sound entirely.
Key Takeaways
- Bypasses damaged hair cells to stimulate the auditory nerve directly.
- Suitable for severe-to-profound hearing loss where aids fail.
- Consists of an external processor and a surgically implanted internal array.
- Requires a dedicated rehabilitation period to "learn" how to hear.
- Modern versions allow for 3.0 Tesla MRI scans without extra surgery.
How the Technology Actually Works
To understand the magic of a cochlear implant, you first have to understand the problem. In a healthy ear, tiny hair cells in the cochlea convert sound waves into electrical impulses. When these cells are destroyed-due to genetics, illness, or loud noise-the chain is broken. Sensorineural Hearing Loss means the "hardware" of the inner ear is failing.
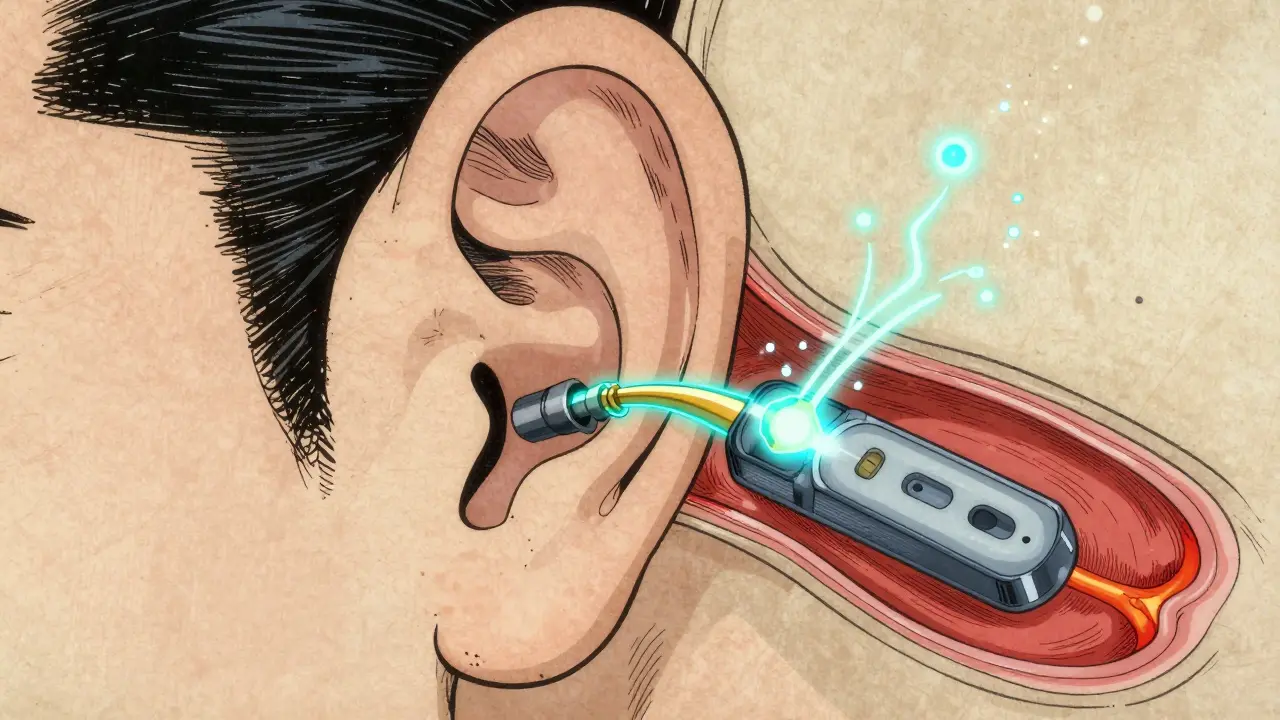
The implant solves this by acting as a bridge. It doesn't try to fix the hair cells; it simply ignores them. The system consists of two main parts: an external piece and an internal piece. The external processor picks up sound and turns it into a digital code. This code is sent through the skin via a magnet to the internal receiver, which then sends electrical pulses directly into the Auditory Nerve. Essentially, it's a digital-to-neural translator.
Breaking Down the Components
It is helpful to think of the system as a team of specialized parts. The external part is the "brain" and the internal part is the "delivery system."
| Component | Location | Primary Function | Key Specification |
|---|---|---|---|
| Sound Processor | External (Behind Ear) | Captures and digitizes sound | 12-22 frequency channels |
| Transmission Coil | External (On Head) | Sends data via inductive coupling | 5-10 MHz radio frequency |
| Receiver-Stimulator | Internal (Under Skin) | Converts data to electrical pulses | Approx. 4-5 cm diameter |
| Electrode Array | Internal (In Cochlea) | Directly stimulates the nerve | 12-22 individual contacts |
The Surgical Process: What Happens in the OR?
Getting an implant isn't like getting a hearing aid; it's a full-scale surgical procedure. While it might sound intimidating, the process is highly standardized and usually takes about two hours per ear. The surgeon starts with a small incision behind the ear to access the mastoid bone. Through a process called a mastoidectomy, they create a path to the middle ear.
The most critical part is the insertion of the electrode array. The surgeon must carefully place these electrodes into the Scala Tympani (a fluid-filled canal in the cochlea). To ensure safety, doctors use facial nerve monitoring-basically an electrical check-to make sure they don't accidentally touch the nerve that controls your face. The receiver is then tucked into a shallow pocket in the skull, keeping it secure and flush against the bone.
The "Activation" and the Road to Hearing
Here is the part that surprises most people: you don't hear anything immediately after surgery. You have to wait about two to four weeks for the swelling to go down and the tissue to heal. This is called the "activation" phase. When the processor is first turned on, the sounds aren't "natural." Most users describe the first few days as hearing "robotic" or "mechanical" noises. This is because your brain has forgotten how to process sound, or if you're a child, it has never learned.
Rehabilitation is where the real work happens. For adults, it's about mapping the new sounds to known words. For children, especially those implanted before age two, the goal is to integrate the device into their natural language development. With intensive auditory-verbal therapy, many children can achieve speech levels that are nearly indistinguishable from their hearing peers. However, for those implanted later in life, the journey is more about functional communication-learning to navigate a conversation in a quiet room before tackling a noisy restaurant.
Comparing Implants vs. Hearing Aids
It's a common mistake to think these two are just different "levels" of the same thing. They are fundamentally different technologies. A hearing aid is an amplifier; it's like a megaphone for your ear. If your auditory nerve is dead, a megaphone doesn't help because there's no one there to hear the message.
Data from the Cleveland Clinic shows a stark difference in outcomes for those with profound loss. While less than 20% of profoundly deaf adults gain significant sentence recognition with hearing aids, about 80% of cochlear implant recipients reach 80% or better recognition in quiet settings. But there's a trade-off: music. Because implants stimulate the nerve in "chunks" rather than a smooth wave, music often sounds flat or distorted. You can hear the beat and the melody, but the richness of a symphony is often lost.

Who is a Good Candidate?
Not everyone with hearing loss needs an implant. In fact, if you have a non-functional auditory nerve, an implant won't work because there's no "wire" to send the signal to the brain. In those cases, a Bone Conduction Device might be a better alternative.
Generally, candidates fall into these groups:
- People with severe-to-profound sensorineural loss in both ears.
- Individuals who get little to no benefit from high-powered hearing aids.
- Children as young as 9-12 months who are identified early with profound deafness.
- Adults with single-sided deafness who want to restore awareness in their "silent" ear.
Modern Advances and the Future
The technology is moving fast. One of the biggest headaches for old-school implant users was getting an MRI. Because the internal magnets could shift under the powerful magnetic field of an MRI machine, patients often had to have a second surgery to remove the magnet before the scan. Newer systems, like the SYNCHRONY 2, have solved this, allowing for 3.0 Tesla MRI scans without any extra surgical intervention.
We are also seeing the rise of "hybrid" devices. These are for people who can still hear low-frequency sounds but are deaf to high frequencies. The device uses a hearing aid for the lows and an electrical implant for the highs. Looking ahead, the integration of Artificial Intelligence (AI) into the external processors will likely help users filter out background noise more effectively, making a crowded coffee shop feel less like a wall of static.
Does a cochlear implant restore "normal" hearing?
No, it doesn't. It restores the ability to hear and understand speech, but the sound quality is different from natural hearing. Many users describe it as a bit more mechanical or electronic, and it takes time for the brain to adapt to this new type of input.
How long do the implants last?
The internal components are designed to last for decades, often 20-30 years. The external sound processor is more like a piece of consumer electronics; it can be upgraded or replaced as the technology improves without needing another surgery.
Is the surgery dangerous?
Like any surgery, it has risks, but complication rates are generally low (below 5%). Major complications, such as facial nerve injury, occur in less than 1% of cases thanks to modern monitoring equipment.
Can children get cochlear implants?
Yes, they are FDA-approved for children as young as 9 to 12 months. Early implantation is crucial because it allows the child to develop language skills during the critical window of brain development.
What happens if the device fails?
While rare, about 5-10% of recipients may experience a device failure. Depending on whether the issue is with the external processor or the internal electrode, this might require a simple replacement of the external unit or a revision surgery for the internal part.
Next Steps and Troubleshooting
If you or a loved one is considering this path, the first step is a comprehensive evaluation by a multidisciplinary team. This usually includes an otolaryngologist (ENT doctor) and an audiologist. They will perform a series of tests to ensure your auditory nerve is functional enough to support an implant.
For those who have already had surgery and are struggling with sound quality, remember that "mapping" is an ongoing process. Your audiologist can adjust the electrical thresholds of the electrodes to make sounds more comfortable. If you experience persistent dizziness or a new ringing in the ears (tinnitus), contact your surgical team immediately, as these can be signs that need professional adjustment.








Write a comment